What is Autism?
Autism is a lifelong neurodevelopmental difference affecting the way a person communicates and interacts with others, how information is processed and how the person makes sense of the world.
What is autism?
As with all people, each autistic person has their own unique profile of strengths, abilities and challenges. For this reason, it is important that approaches to support are responsive to the individual. There are however, some common threads underlying the autistic experience which it can be helpful to consider when planning for support. The Scottish Government Different Minds website was created in partnership with autistic people:
‘Autism is part of everyday life. Yet even though 1 in 100 people in Scotland are autistic, it’s often misunderstood. Autism is a neurological difference; put simply, autistic brains work differently to non-autistic brains. They see and experience the world differently to non-autistic people. It’s important that we understand more about autism – both what it is, and what it is not.’ https://differentminds.scot/
Their campaign video offers a brief introduction to autism:
Whilst every individual is unique, there are some core features which are common to the autistic experience. As illustrated in the image below, these include:
- Communication differences
- Sensory differences
- Thinking differences
- Impact of Environment
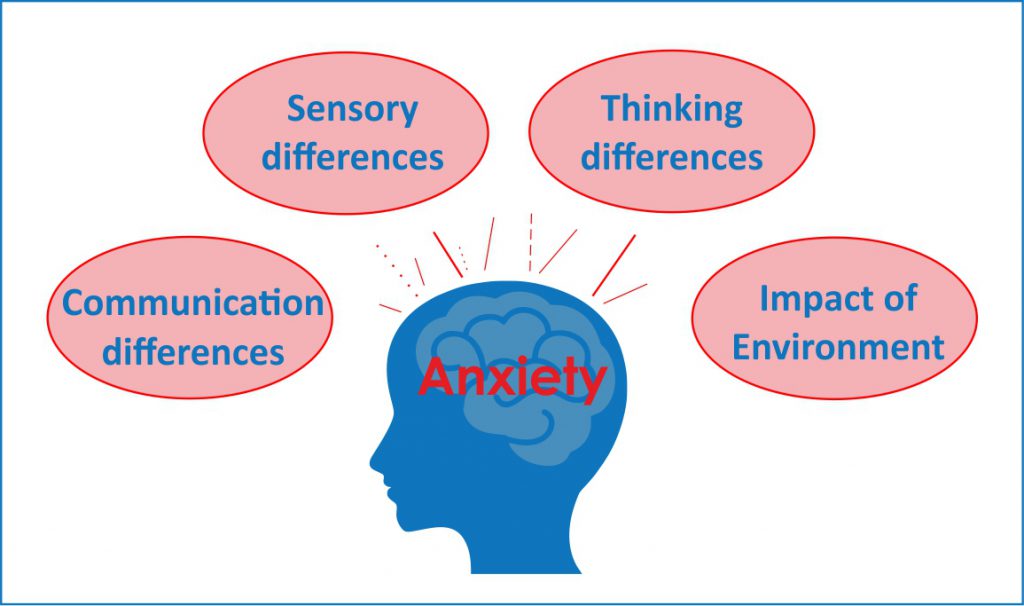
If these four aspects are not appropriately supported, an autistic person can experience anxiety and distress. For children and young people, there is a reciprocal relationship between the autistic learner and the environment – this includes the physical environment and the people around them. With appropriate understanding and adjustments autistic people can flourish.
Autism is not a linear scale running from ‘high functioning’ to ‘low functioning’, which are unhelpful terms. Instead, autism varies in several different ways – sensory differences, levels of anxiety, social skills and executive functions all vary both from person to person and from time to time. This short comic strip provides one explanation.
Children and young people’s development may progress at a different pace to their peers. Children and young people may experience difficulties across different areas, including:
- Building independence
- Motor skills
- Social communication
- Play/flexibility
- Sensory/regulation
- Academic and learning
- Attention, memory, organisation and planning
- Emotional wellbeing/mental health
- Attachment and relationships
Sometimes children developing differently may need a bit of extra support from the people around them, or some changes to their environment to help them to achieve their potential. Simple adaptations can make things easier. For some people, however, they may continue to need a lot of support, even with adaptations.
Autism and Neurodiversity (click here)
Neurodiversity is a relatively new term, thought to have been coined in the 1990s by Judy Singer (an autistic individual, parent of an autistic child and Sociologist). It was originally used by the autistic community, who were keen to move away from the medical model and dispel the belief that autism is something to be treated and cured rather than an important and valuable part of human diversity.
The idea of neurodiversity has now been embraced by many other groups, who are using the term as a means of empowerment and to promote the positive qualities possessed by those with a neurodevelopmental difference. It encourages people to view neurodevelopmental differences such as autism, dyslexia and dyspraxia as natural and normal variations of the human genome. Furthermore, it encourages them to reject the culturally entrenched negativity which has typically surrounded those that live, learn experience the world in a particular way that is sometimes perceived as different.
The whole of society is neurodiverse. Diversity is the trait of a whole group not of an individual. It is estimated that around 1 in 7 people (more than 15% of people in the UK) have neurodevelopmental differences, including autism, which are observed when they learn and process information in a particular way.
The human population is highly diverse. Neurodiversity is a term that is increasingly used to describe this normal variation across all people. Within the autistic population there is also a great deal of diversity and autism manifests differently from one individual to another.
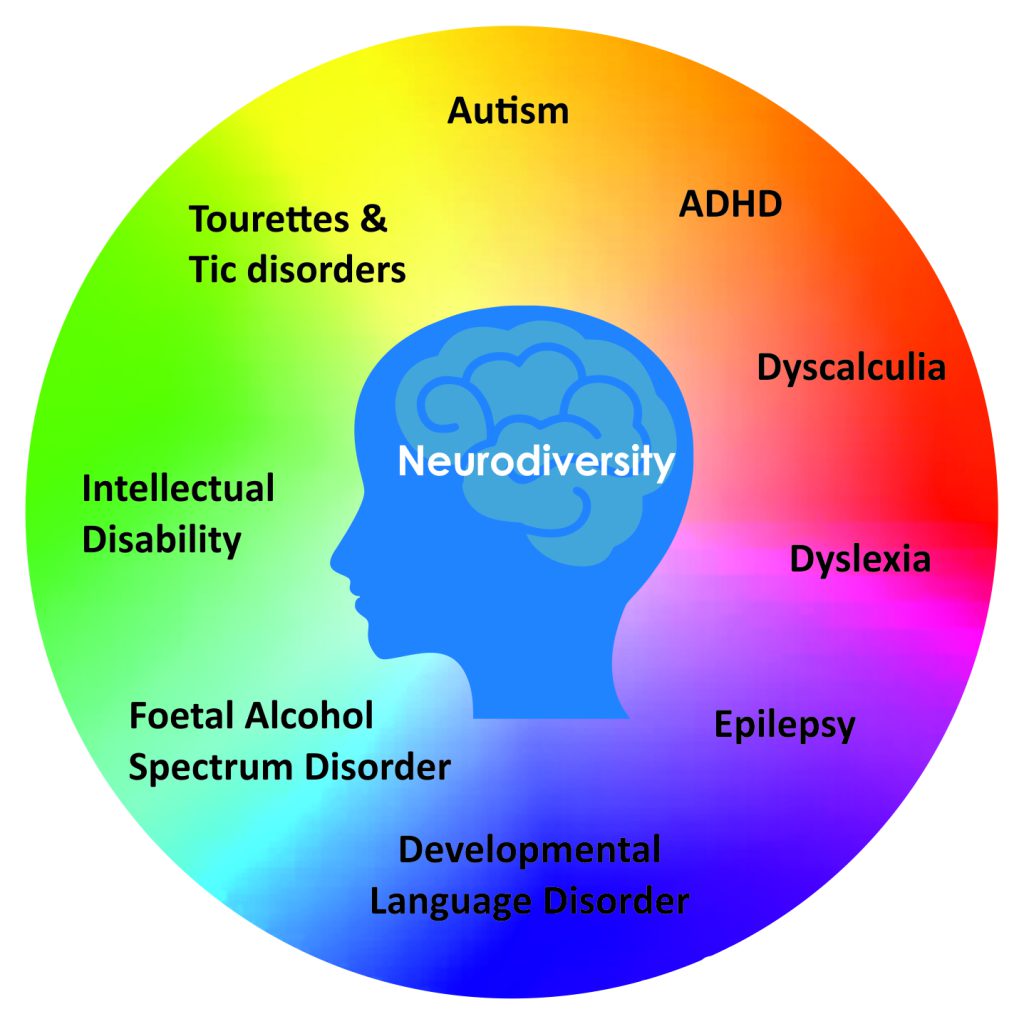
Autism often co-occurs with other neurodevelopmental differences including;
- Attention Deficit Hyperactivity Disorder (ADHD)
- Developmental Co-ordination Disorder (DCD) also referred to as Dyspraxia
- Developmental Language Disorder (DLD)
- Epilepsy
- Foetal Alcohol Spectrum Disorder
- Intellectual Disability
- Tourettes and Tic disorders
- Specific Learning Disorder/ Differences e.g Dyslexia, Dyscalculia
Many neurodevelopmental difficulties overlap and interact. These conditions are often identified and diagnosed during childhood or adolescence. Symptoms and behaviours often change as a child grows older, with some difficulties being more long-standing. For some children and young people, some areas of difficulty may become more noticeable and have an increasing impact on their daily lives as they get older.
How common is autism? (click here)
Autism affects around 1.03 % of the Scottish population (Colvin et al 2021).
There are some groups where autism is under-recognised for example:
- Females
- Black and minority ethnic children and young people
- Children living in poverty
Around 4% of children who are referred for autism assessments because they have similar presentations, do not receive a diagnosis of autism, however they are still entitled to support to ensure their needs are met.
Autism is thought to be more common in boys than girls, however there is a growing consensus that many girls are under-diagnosed or misdiagnosed. A range of reasons are given for this, including different societal expectations; diagnostic tools being designed around boys; special interests are often determined by gender due to societal expectations and interests of girls might be perceived as less unusual (for example, a strong interest in lip balms compared with an interest in trains).
Useful links about under-recognised groups
Rutherford, M., McKenzie, K., Johnson, T., Catchpole, C., O’Hare, A., McClure, I.,. & Murray, A. (2016). Gender ratio in a clinical population sample, age of diagnosis and duration of assessment in children and adults with autism spectrum disorder. Autism, 20(5), 628-634.
Baird, G., Douglas, H. R., & Murphy, M. S. (2011). Recognising and diagnosing autism in children and young people: summary of NICE guidance. BMJ, 343, d6360.
Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., & Charman, T. (2006). Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). The lancet, 368(9531), 210-215.
What causes autism? (click here)
For most individuals the cause of autism is not identified. Autism is generally thought to have a genetic basis and research is ongoing.
Find out more on the National Autistic Society website: The causes of autism
Learning/intellectual disability and autism (click here)
Intellectual disability and autism
According to the Scottish Government (2021), approximately 32.7% of individuals with an intellectual disability also have a diagnosis of autism.
Autism is a lifelong neurodevelopmental condition or difference which affects how an individual processes information and communicates. There are some common threads underlying the autistic experience which it can be helpful to consider when planning for support:
- differences in developmental trajectory
- differences in communication style
- difference in thinking style and processing of information
- an ability to become deeply absorbed in specific interests
- over- or under-sensitivity to the sensory environment
- a positive response to routines and predictability
Whilst there are several similarities and overlaps of need between autism and intellectual disability, they are not always exactly the same. This has caused some confusion when separating out recommendations, and when multiagency input is required e.g. between health, social care and education. Because of this challenge, it is important that approaches to support are responsive to the individual.
Autism and gender (click here)
Autism is thought to be more common in boys than girls, however there is a growing consensus that girls are under diagnosed or misdiagnosed. A range of reasons are given for this, including different societal expectations; diagnostic tools being designed around boys; special interests are often gender determined due to social expectations and interests of girls might be perceived as less unusual (e.g. strong interest in lip balms compared with interest in trains).
The quiet, anxious presentation of autism occurs across genders but might be more prevalent in girls and these individuals are more likely to be missed.
Further information and resources
Rutherford, M., McKenzie, K., Johnson, T., Catchpole, C., O’Hare, A., McClure, I., … & Murray, A. (2016). Gender ratio in a clinical population sample, age of diagnosis and duration of assessment in children and adults with autism spectrum disorder. Autism, 20(5), 628-634.
Habayeb, S., Kenworthy, L., De La Torre, A. et al. (2022). Still Left Behind: Fewer Black School-Aged Youth Receive ASD Diagnoses Compared to White Youth. J Autism Dev Disord 52, 2274–2283. https://link.springer.com/article/10.1007/s10803-021-05118-1 Is open access, freely available PDF copy to download.
Morgan-Trimmer, R. (2022). Autism in women – under-diagnosed, under-served and under-represented. Murmations: Journal of Transformative Systemic Practice, 4 (2), 10 – 19. http://murmurations.cloud/ojs/index.php/murmurations/article/view/158 Is open access with freely available PDF copy to download.